.jpg)


ESTROGEN INCREASES THE SECRETION OF GH IN RESPONSE TO STIMULATION: CHILD AND YOUTH.
THE STIMULATION OF GROWTH HORMONE RELEASE-GH AND SUMMARY ESTROGEN IN CHILD, INFANT AND JUVENILE, THE POTENTIAL EFFECT OF ESTROGEN IN CONTROL OF GH SECRETION IN ANTERIOR PITUITARY CELLS: PHYSIOLOGY-ENDOCRINOLOGY-NEUROENDOCRINOLOGY-GENETICS-ENDOCRINE-PEDIATRICS (SUBDIVISION OF ENDOCRINOLOGY): DR. JOÃO SANTOS CAIO JR ET DRA HENRIQUETA VERLANGIERI CAIO.
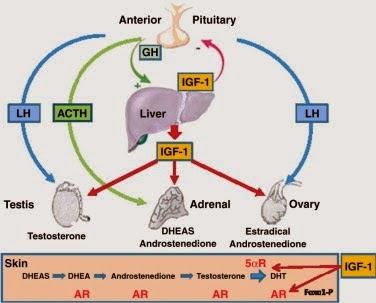
The GH-growth hormone plays a central role in the regulation of body growth and development growth beyond the longitudinal, linear in juvenile, infant, child and adolescent, which is modulated by sex steroids. A presence with interaction between estrogen and GH leads to obtaining gender specific body composition during puberty. Most previous studies have focused on the effects of estrogen on GH secretion. There is also strong evidence that estrogen modulates GH action independent of secretion. The metabolic action of GH in the liver, causing a decrease in the production of IGF-I and fat oxidation in general is present. This results in a loss of lean tissue and a gain of body fat in postmenopausal women and there is an analogy in a GHD effect in women with hypopituitarism replacing GH. The hypopituitarism is an endocrine disorder characterized by decreased secretion of one or more of the eight hormone normally produced by the pituitary (hypophyses), in the base of the brain.

Dr. João Santos Caio Jr.
Endocrinologia – Neuroendocrinologista
CRM 20611
Dra. Henriqueta V. Caio
Endocrinologista – Medicina Interna
CRM 28930
1. Proteínas de ligação de GH (GHBPs) GHBP-Growth Hormone-Binding Protein (Proteína ligadora do hormônio de crescimento) estão presentes no sangue de várias espécies e por complexação com circulação de GH hormônio de crescimento pode alterar a sua recarga e distribuição...
http://hormoniocrescimentoadultos.blogspot.com
2. As ações de GHBP-Growth Hormone-Binding Protein humana (hGHBP) até agora têm sido estudados indiretamente, através de seus efeitos sobre a liberação de hGH...
http://longevidadefutura.blogspot.com
3. As reações de complexação que são aquelas em que se formam complexos e fazem parte da complexometria...
http://imcobesidade.blogspot.com
AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO
DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA.
Referências Bibliográficas:
Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Rose SR, Ross JL, Uriarte M, Barnes KV, Cassorla FG, Cuttler Jr GB. The advantage of measuring stimulated as compared with spontaneous growth hormone levels in the diagnosis of growth hormone deficiency. N Engl J Med. 1988; 319:201-207; Donaldson DL, Pan F, Hollowell JG, Stevenson JL, Gifford AR, Moore WV. Reliability of stimulated and spontaneous growth hormone (GH) levels for identifying the child with low GH secretion. J Clin Endocrinol Metab. 1991; 72:647- 652; Rosenfeld RG, Albertsson-Wikland K, Cassorla F, Fraiser SD, Haseqaua Y, Hintz RL, LaFranchi S, Lippe B, Lauriaux L, Melmed S. Diagnostic controversy: the diagnosis of childhood growth hormone deficiency revisited. J Clin Endocrinol Metab. 1995; 801:1532-1540; Ghigo E, Bellone J, Aimaretti G, Bellone S, Loche S, Cappa M, Bartolotta E, Dammacco F,Camanni F. Reliability of provocative tests to assess growth hormone secretory status. Study in 472 normally growing children. J Clin Endocrinol Metab. 1996; 81 :3323- 327; Saggese G, Ranke MB, Saenger P, Rosenfeld RG, Tanaka T, Chaussain JL, Savage MO. Diagnosis and treatment of growth hormone deficiency in children and adolescents: towards a consensus. Horm Res. 1998; 50:320-340; Shalet SM, Toogood A, Rahim A, Brennan BMD. The diagnosis of growth hormone deficiency in children and adults. Endocr Rev. 1998; 19:203-223; GH Research Society: Consensus guidelines for the diagnosis and treatment of growth hormone (GH) deficiency in childhood and adolescence: summary statement of the GH research society. J Clin Endocrinol Metab. 2000; 85:3990-3993. Rosenfeld RG. Editorial: is growth hormone deficiency a viable diagnosis? J Clin Endocrinol Metab. 1997; 82:349 -355; Juul A, Bernasconi S, Clayton PE, Kiess W, DeMuinck-Keizer Schrama S; Drugs and Therapeutics Committee of the European Society for Paediatric Endocrinology (ESPE). European audit of current practice in diagnosis and treatment of childhood growth hormone deficiency. Horm Res. 2002; 58:233-241; Wyatt DT, Mark D, Slyper A. Survey of growth hormone treatment practices by 251 pediatric endocrinologist. J Clin Endocrinol Metab. 1995; 80:3292-3297. Gourmelen M, Pham-Trung M, Girard F. Transient partial hGH deficiency in prepubertal children with delay of growth. Pediatr Res. 1979;13:221-224; Clayton PE, Price DA, Shalet SM. Growth hormone state after completion of treatment with growth hormone. Arch Dis Child. 1987; 62:222- 226.
Site Van Der Häägen Brazil
www.vanderhaagenbrazil.com.br
www.clinicavanderhaagen.com.br
www.crescimentoinfoco.com
www.obesidadeinfoco.com.br
http://drcaiojr.site.med.br
http://dracaio.site.med.br
João Santos Caio Jr
http://google.com/+JoaoSantosCaioJr
Vídeo
http://youtu.be/woonaiFJQwY
Google Maps:
http://maps.google.com.br/maps/place?cid=5099901339000351730&q=Van+Der+Haagen+Brasil&hl=pt&sll=-23.578256,46.645653&sspn=0.005074,0.009645&ie=UTF8&ll=-23.575591,-46.650481&spn=0,0&t = h&z=17
Referências Bibliográficas:
Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Rose SR, Ross JL, Uriarte M, Barnes KV, Cassorla FG, Cuttler Jr GB. The advantage of measuring stimulated as compared with spontaneous growth hormone levels in the diagnosis of growth hormone deficiency. N Engl J Med. 1988; 319:201-207; Donaldson DL, Pan F, Hollowell JG, Stevenson JL, Gifford AR, Moore WV. Reliability of stimulated and spontaneous growth hormone (GH) levels for identifying the child with low GH secretion. J Clin Endocrinol Metab. 1991; 72:647- 652; Rosenfeld RG, Albertsson-Wikland K, Cassorla F, Fraiser SD, Haseqaua Y, Hintz RL, LaFranchi S, Lippe B, Lauriaux L, Melmed S. Diagnostic controversy: the diagnosis of childhood growth hormone deficiency revisited. J Clin Endocrinol Metab. 1995; 801:1532-1540; Ghigo E, Bellone J, Aimaretti G, Bellone S, Loche S, Cappa M, Bartolotta E, Dammacco F,Camanni F. Reliability of provocative tests to assess growth hormone secretory status. Study in 472 normally growing children. J Clin Endocrinol Metab. 1996; 81 :3323- 327; Saggese G, Ranke MB, Saenger P, Rosenfeld RG, Tanaka T, Chaussain JL, Savage MO. Diagnosis and treatment of growth hormone deficiency in children and adolescents: towards a consensus. Horm Res. 1998; 50:320-340; Shalet SM, Toogood A, Rahim A, Brennan BMD. The diagnosis of growth hormone deficiency in children and adults. Endocr Rev. 1998; 19:203-223; GH Research Society: Consensus guidelines for the diagnosis and treatment of growth hormone (GH) deficiency in childhood and adolescence: summary statement of the GH research society. J Clin Endocrinol Metab. 2000; 85:3990-3993. Rosenfeld RG. Editorial: is growth hormone deficiency a viable diagnosis? J Clin Endocrinol Metab. 1997; 82:349 -355; Juul A, Bernasconi S, Clayton PE, Kiess W, DeMuinck-Keizer Schrama S; Drugs and Therapeutics Committee of the European Society for Paediatric Endocrinology (ESPE). European audit of current practice in diagnosis and treatment of childhood growth hormone deficiency. Horm Res. 2002; 58:233-241; Wyatt DT, Mark D, Slyper A. Survey of growth hormone treatment practices by 251 pediatric endocrinologist. J Clin Endocrinol Metab. 1995; 80:3292-3297. Gourmelen M, Pham-Trung M, Girard F. Transient partial hGH deficiency in prepubertal children with delay of growth. Pediatr Res. 1979;13:221-224; Clayton PE, Price DA, Shalet SM. Growth hormone state after completion of treatment with growth hormone. Arch Dis Child. 1987; 62:222- 226.
Contato:
Rua
Estela, 515 - Bloco D - 12º andar - Conj 121/122
Paraiso - São Paulo - SP - Cep 04011-002.
Paraiso - São Paulo - SP - Cep 04011-002.
Site Van Der Häägen Brazil
www.vanderhaagenbrazil.com.br
www.clinicavanderhaagen.com.br
www.crescimentoinfoco.com
www.obesidadeinfoco.com.br
http://drcaiojr.site.med.br
http://dracaio.site.med.br
João Santos Caio Jr
http://google.com/+JoaoSantosCaioJr
Vídeo
http://youtu.be/woonaiFJQwY
Google Maps:
http://maps.google.com.br/maps/place?cid=5099901339000351730&q=Van+Der+Haagen+Brasil&hl=pt&sll=-23.578256,46.645653&sspn=0.005074,0.009645&ie=UTF8&ll=-23.575591,-46.650481&spn=0,0&t = h&z=17